
碳离子放射治疗眼眶恶性肿瘤3例并文献复习
碳离子放射治疗眼眶恶性肿瘤3例并文献复习
芦静,李小军*,柴鸿钰,王艳
甘肃省武威肿瘤医院(兰州院区)重离子放疗病区 甘肃 兰州 730000
第一作者:芦静(1988-07-26)女,汉族,本科,主治医师,研究方向:肿瘤放射治疗,邮箱:m18209456698@163.com
*通讯作者:李小军(1982-05-04)男,汉族,本科,主任医师,研究方向:肿瘤放射治疗,邮箱:anglwe@sina.com
摘要 目的:探讨3例眼眶恶性肿瘤碳离子放射治疗(CIRT)的疗效及安全性。方法:回顾性分析2022年7月至 2023 年7月于甘肃省武威肿瘤医院接受CIRT治疗的3例眼眶恶性肿瘤患者的临床资料,并复习相关文献。结果:3例患者均完成CIRT治疗,平均随访20.5个月(15-26个月)。病例1经CIRT治疗后3个月达到完全缓解(CR),病例2经CIRT治疗后3个月达到CR,病例3经CIRT治疗后12月达到部分缓解(PR)。3例患者的1年局部控制率(LC)、1年无进展生存率(PFS)、1年总生存率(OS)均为 100.0%。1例患者发生1级放射性结膜损伤,2例患者发生1级放射性皮肤反应,1例患者发生1级眼干的放疗晚期不良反应;所有患者均未发生2级及以上的不良反应。结论: CIRT应用于不可手术切除、术后残留及复发的眼眶恶性肿瘤可获得良好的OS和 LC,且急性和晚期毒性反应较少。
关键词: 碳离子放疗;眼眶恶性肿瘤;疗效
3 cases of orbital malignant tumor treated with carbon ion radiotherapy and literature review
LU Jing, LI Xiao-jun*, CHAI Hong-yu, WANG Yan
Department of Heavy Ion Radiotherapy, Lanzhou Branch of Wuwei Cancer Hospital of Gansu, Lanzhou, Gansu, 730000, China
ABSTRACT Objective: To investigate the efficacy and safety of carbon ion radiotherapy (CIRT) in 3 cases of orbital malignant tumors. Methods: The clinical data of 3 patients with orbital malignant tumor who received CIRT treatment in Wuwei Cancer Hospital of Gansu Province from July 2022 to July 2023 were retrospectively analyzed, and the relevant literature was reviewed. Results: Three patients completed CIRT treatment, they were followed up for an average of 20.5 months (15-26 months). Case 1 achieved complete response (CR) 3 months after CIRT treatment, case 2 achieved CR 3 months after CIRT treatment, and case 3 achieved partial response (PR) 12 months after CIRT treatment. The 1 year local control rate (LC), 1-year progression-free survival (PFS), and 1-year overall survival (OS) of the three patients were 100.0%. One patient had grade 1 radiation conjunctival injury, 2 patients had grade 1 radiation skin reaction, and 1 patient had grade 1 dry eye late adverse reaction. No adverse reactions of grade 2 or higher occurred in all patients. Conclusion: The application of CIRT in unresectable, postoperative residual and recurrent orbital malignant tumors can obtain good OS and LC, and acute and late toxic reactions are less.
Key words: Carbon ion radiotherapy; Orbital malignant tumor; Curative effect
前言
眼眶恶性肿瘤眼起源于眼眶内的病变,其发病率为3.4/106人/年,占所有肿瘤的0.1%,占所有眼部疾病的不到20%[1-2]。眼眶解剖结构复杂,眼眶内组织可来源于表皮外胚层、中胚层及神经外胚层等,因此眼眶恶性肿瘤的种类繁多,分类复杂,病情进展迅速,不仅影响患者的视力和外观,还可能出现远处转移甚至导致患者死亡[3-4]。手术是治疗眼眶恶性肿瘤的主要治疗方法,由于手术切缘阳性或近切缘、淋巴结阳性、神经周围浸润、肿瘤为局部晚期等,完整切除眼眶恶性肿瘤较难实现,因此针对眼眶恶性肿瘤术后患者和无法行手术切除的患者,通常给予放疗、化疗等综合治疗[5-6]。调强放疗(IMRT)是眼眶恶性肿瘤患者术后及无法行手术切除患者的常用辅助治疗,但放疗诱导的毒性限制IMRT对肿瘤靶点的剂量,由于光束路径的入口和出口剂量过高,造成肿瘤剂量覆盖困难及使得周边正常组织体积剂量较高,影响疗效[7]。低剂量通常不足以控制包括鳞状细胞癌、腺样囊性癌(ACC)和软组织肉瘤(STS)等常见的眼眶恶性肿瘤病情[8]。因此有必要探寻一种更有效、副作用更低的治疗技术以突破目前眼眶恶性肿瘤的治疗瓶颈。本研究回顾性分析3例眼眶肿瘤患者的临床资料及接受碳离子放射治疗(CIRT)治疗的疗效和安全性,并复习相关文献加深对该治疗方式及疗效的认识。
1、临床资料
病例1:女性,44岁,右侧泪囊鳞癌。于2022年7月就诊我院,查体见右眼下眼睑大小约3cm×4cm肿物,眼球运动各方向轻度受限。经过对患者全面检查和评估,患者于2022年7月20日接受CIRT治疗。一程处方剂量:PTV 40Gy(RBE)/10fx;侧卧位,2D均匀扫描,剂量分布见图1A。二程处方剂量:PTVboost 24Gy(RBE)/6fx;仰卧位,2D均匀扫描。肿瘤区总剂量为 64 Gy (RBE)/16 F,4.0 Gy (RBE) /F,5 F/w,剂量分布见图1B。CIRT和容积调强放射治疗(VMAT)计划在均满足处方要求的前提下,轴位图像剂量分布的对比,周围正常组织CIRT计划较VMAT计划低剂量照射范围明显缩小,见图2A和图2B。CIRT治疗前、后通过影像学资料对比疗效,根据实体瘤疗效评价标准(RECIST)1.1评估患者疗效,治疗后3个月,疗效达完全缓解(CR),见图3。CIRT治疗期间及治疗后1月内,患者出现1级急性放射性结膜损伤;于放疗结束3个月后出现眼干,长期使用滴眼液,考虑为1级放射性结膜损伤(RTOG急性放射损伤分级),未观察到大于2级的晚期不良反应。CIRT治疗期间联合使用靶向(西妥昔单抗),治疗期间出现面部散发皮疹,不良事件通用术语评价标准1级。截至2024年9月,目前患者无病状态,继续长期随访。
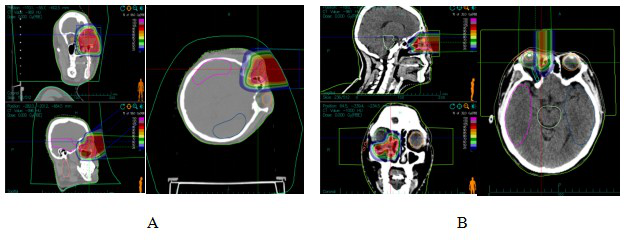
图1泪囊鳞癌CIRT治疗剂量分布图
Figure 1 CIRT dose distribution in patients with dacryocystosquamous cell carcinoma
Note: Figure 1A: One course CIRT dose distribution. Figure 1B: Two course CIRT dose distribution

图2 泪囊鳞癌患者VMAT计划及碳离子计划剂量分布图
Figure 2 VMAT plan and carbon ion plan dose distribution in patients with dacryocystosquamous cell carcinoma
Note: Figure 2A: VMAT plan dose distribution in patients with dacryocystosquamous cell carcinoma. Figure 2B: Carbon ion plan dose distribution in patients with dacryocystosquamous cell carcinoma.
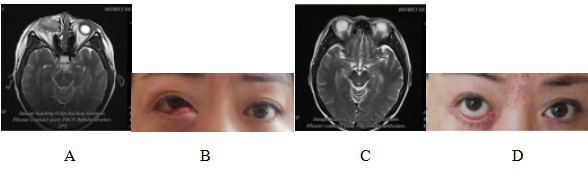
图 3 泪囊鳞癌患者CIRT治疗前后磁共振成像(MRI)及体征对比图
Figure 3 Comparison of magnetic resonance imaging (MRI) and physical signs in patients with dacryocystosquamous cell carcinoma before and after CIRT treatment
Note: Figure 3A: MRI examination before CIRT treatment showed that: the right lacrimal sac was occupied, the boundary between the eyeball, the medial rectus muscle and the inferior rectus muscle was not clear, the eyeball was compressed and displaced, and the right nasolacrimal duct was invaded. Figure 3B: Abnormal signs before CIRT treatment; Figure 3C: MRI examination after CIRT treatment showed that: the lesion disappeared, and the efficacy evaluation was CR; Figure 3D: Recovery of physical signs after CIRT treatment.
病例2:男性,38岁,右眼脉络膜恶性黑色素瘤。于2023年4月就诊于我院,眼底检查见视盘界清色淡红,网膜颞下象限可见一棕黑色高隆起性肿物,肿物周边继发性视网膜脱离,波及黄斑区。经过对患者全面检查和评估,患者于2023年4月25日至5月12日接受CIRT治疗。处方剂量为:PTV 70Gy/14Fx,5GyE/Fx。仰卧位,2D均匀扫描技术,剂量分布见图4。CIRT和VMAT计划在均满足处方要求的前提下,在轴位图像剂量分布的典型对比,周围正常组织CIRT计划较VMAT计划低剂量照射范围明显缩小,见图5。治疗期间给予患者特瑞普利单抗注射液(240毫克)免疫治疗2周期。CIRT治疗前、后通过影像学资料对比疗效,根据RECIST1.1肿瘤疗效评价标准评估患者疗效,治疗后3个月疗效为CR,见图6。CIRT治疗期间及治疗后1月内,患者出现1级放射性皮肤损伤,视力同前,未观察到大于2级的不良反应,治疗后3个月视力改善。截至2024年9月,目前患者无病状态,继续长期随访。
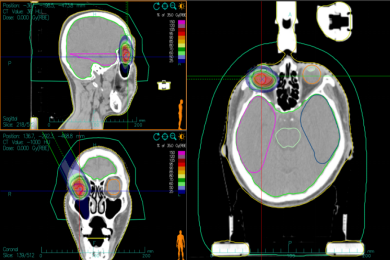
图4 脉络膜恶性黑色素瘤患者CIRT治疗剂量分布图
Figure 4 CIRT dose distribution in patients with malignant choroidal melanoma
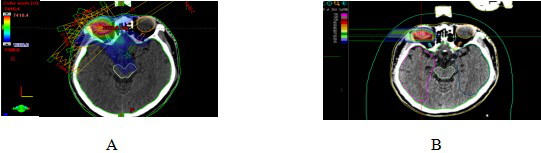
图5脉络膜恶性黑色素瘤患者VMAT计划及碳离子计划剂量分布图
Figure 5 VMAT plan and carbon ion plan dose distribution in patients with malignant choroidal melanoma
Note: Figure 5A: VMAT plan dose distribution in patients with malignant choroidal melanoma. Figure 5B: Carbon ion plan dose distribution in patients with malignant choroidal melanoma.
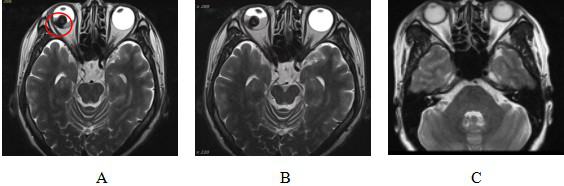
图6脉络膜恶性黑色素瘤患者CIRT治疗前后MRI对比
Figure 6 Comparison of MRI before and after CIRT treatment for malignant melanoma of choroid
Note: Figure 6A: MRI examination results before CIRT treatment showed: Abnormal signal nodules on the right side of the base of the eyeball. The red circle shows the extent of tumor invasion.
Figure 6B: MRI results after CIRT treatment showed: Abnormal signal nodules on the right lateral temporal side of the base of the eyeball, with little change compared with before.
Figure 6C: MRI examination 90 days after CIRT treatment showed that: the lesion disappeared and the efficacy was evaluated as CR.
病例3:女性,59岁,右眼眶ACC术后。于2023年4月四川大学华西医院行“右眼眶内肿物切除+眼眶修补术”,术后病检提示:ACC。术后1月就诊于我院,目前患者眼睑闭合、右眼外转和下转明显受限。经过对患者全面检查和评估,患者于2023年6月12日接受CIRT治疗,一程处方剂量为PTVboost:15Gy(RBE)/5fx。二程处方剂量为PTV:54Gy(RBE)/18fx,肿瘤总剂量达到69Gy(RBE)/23fx,剂量分布见图7。CIRT和VMAT计划在均满足处方要求的前提下,在轴位图像剂量分布的典型对比,周围正常组织CIRT计划较VMAT计划低剂量照射范围明显缩小,见图8。CIRT治疗前、后通过影像学资料对比疗效,根据RECIST1.1肿瘤疗效评价标准评估患者疗效,疗效达部分缓解(PR),见图9。CIRT治疗期间及治疗后1月内,患者出现1级放射性皮肤损伤,未观察到大于2级的不良反应。截至2024年7月,目前患者带瘤生存,继续长期随访。
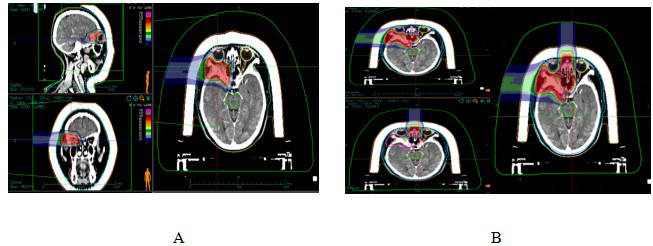
图7 眼眶ACC患者离子治疗剂量分布图
Figure 7 Ion therapy dose distribution in orbital ACC patients
Note: Figure 7A: One course CIRT dose distribution. Figure 7B: Two course CIRT dose distribution
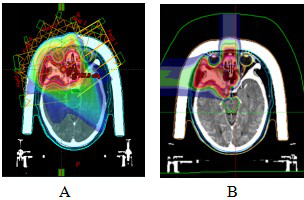
图8 眼眶ACC患者VMAT计划及碳离子计划剂量分布图
Figure 8 VMAT plan and carbon ion plan dose distribution in orbital ACC patients
Note: Figure 8A: VMAT plan dose distribution n orbital ACC patients. Figure 8B: Carbon ion plan dose distribution n orbital ACC patients.
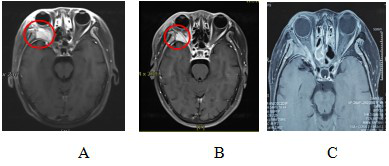
图9 眼眶ACC患者CIRT治疗前后MRI对比
Figure 9 Comparison of MRI before and after CIRT treatment for orbital ACC patients
Note: Figure 9A: MRI examination before CIRT treatment showed that: the right orbital space was occupied, and the boundary between the right orbital muscle and the external rectus muscle, lacrimal gland, and optic nerve was unclear, and the lateral wall of the orbit was invaded.
Figure 9B: MRI examination after CIRT treatment showed that: the right orbital space was occupied and abnormal enhancement, and the lateral orbital wall was invaded, which was smaller than that of the anterior lesion. The efficacy evaluation was PR.
Figure 9C: MRI examination 12 months after CIRT treatment showed that: the right orbital space was significantly reduced compared with the anterior lesion, and the efficacy evaluation was PR.
2、结果
2.1 疗效评价
3例患者平均随访期20.5个月(15-26个月)。病例1泪囊鳞癌患者CIRT治疗后即达到CR,病例2脉络膜恶性黑色素瘤患者于治疗后3月达到CR,病例3眼眶ACC患者目前随访至1年达到PR。3例患者1年无进展生存率(PFS)为100.0%,1年局部控制率(LC)率为100.0%,1年总生存率(OS)为100.0%。
2.2 安全性评价
所有患者未发生≥2级的放疗相关的不良反应。急性期反应多出现在治疗中和治疗后1月内,表现为放射性皮肤反应和眼损伤。1例发生1级放射性结膜损伤,表现为轻度结膜炎伴有结膜充血,2例发生1级放射性皮肤反应,表现为照射野皮肤色素沉着伴小片状红斑。晚期不良反应方面,观察到1例放射性结膜损伤,表现为眼干、需长期使用滴眼液,出现在放疗结束3个月后。
3、讨论
眼眶肿瘤是一组异质性较大病变,其分类、组织学特征、诊断标准、治疗方法及生存率各不相同。其组织病理学复杂,因生物学行为的差异性,对放化疗敏感性不同,临床预后表现亦不同,部分易出现为局部或区域性复发,部分易表现早期远处转移,故临床治疗方法也存在差异[9-11]。
眼眶恶性肿瘤治疗方法包括手术、辅助放疗、介入、化疗、靶向和免疫治疗等,眼眶手术具有空间狭小、重要的组织结构集中、手术野窄等特点,因此手术难度大、术后并发症多[12-13]。眼眶恶性肿瘤患者因保眼无法获得足够的切缘,根治性手术通常难以实现。眼眶肿瘤患者的放疗仍以光子治疗占主导地位,但大部分眼眶肿瘤(如ACC、视网膜母细胞瘤、恶性黑色素瘤、肉瘤等)光子放疗后常局部复发。一项研究显示,39例眼眶恶性肿瘤患者经手术治疗,其中约20%的患者在中位随访8个月后出现局部复发,3年OS和无复发/无死亡生存率分别为50.5%和47.5%[14]。
近年随着医疗技术的进步,质子和碳离子等一些新型的放疗技术进入大家的视野。一项研究显示[15],22例保眼术后行质子放疗(PRT)和/或CIRT的眼眶肿瘤患者,2年OS、PFS、无远处转移生存率(DMFS)分别为100%、57.9%、72.8%;未观察到急性严重(即≥3级)毒性,严重晚期毒性的发生也很少见。另外,BED(生物效应剂量)可能对DMFS(无远处转移生存率)有显著影响:BED越高,远处转移风险越低。这些发现表明,粒子治疗可能对疾病控制有重大影响。在研究中发现更高的BED与改善的结果相关联,表明CIRT治疗的优势通常体现在邻近危及器官剂量限制的基础上可提高肿瘤剂量,且不增加毒性反应的发生率[16]。
研究表明,放疗剂量超过50Gy,结膜角化,泪腺出现萎缩、纤维化、角膜失代偿。当剂量超过60Gy时,睑粘连、角膜结膜炎、长期的眼睛干涩成了一个问题。此外,约7.0%-20.0%的患者可能发生辐射诱发的视神经病变[17-19]。碳离子束可以通过能量沉积形成布拉格峰,将剂量集中在目标组织内,在杀死靶区肿瘤细胞的同时,尽可能地保护周围和辐射通道上的正常组织,以减少损伤[20-22]。一项研究显示[23],重离子束由于其独特的物理学特性,位于靶区边缘的剂量跌落非常迅速,重离子射束后缘在距95%等剂量线5mm处可衰减70%~80%,在射野后缘1mm的距离,剂量即可衰减8%~19%左右。故碳离子适用于一些毗邻危及器官的靶区进行安全、足量的放射治疗[24-25]。
本研究存在一定局限性。首先,眼眶肿瘤包括一组不同来源的异质性条件,具有本质不同的生物学行为,不同病理相结合必然影响结果的统一性。其次,随访时间有限,因此本研究将继续对这些患者进行随访,并观察远期随访的预后情况。第三,本研究中2例患者采用均匀扫描,1例采用点扫描,在危及器官受量及毒副反应方面可能会有差异。均匀扫描时需制作组织补偿器将落于肿瘤后方的剂量通过补偿器的调节移除,但处于碳离子束入射路径上的部分正常组织也不可避免地受到一定剂量的照射;采用碳离子点扫描技术,通过改变粒子能量改变离子束入射深度,利用笔形束对肿瘤靶区进行三维适形扫描,高剂量分布区(Bragg 峰)被调整嵌合在肿瘤靶区上,射野后缘剂量快速跌落,峰区与坪区之间的RBE值差别最大,使位于坪区的邻近危及器官受量进一步降低。第四,首台国产重离子治疗射野路径固定且射野方向少(垂直、水平),未能充分发挥碳离子的优势,45°射野即将投入使用,有望为头颈部肿瘤尤其是眼眶肿瘤的精确治疗提供更多可能。第五,本研究属于回顾性研究,样本量相对较小,且考虑到本疾病的罕见性,目前几乎已发表的文献均来自单一机构的回顾性研究。若无专业学术中心之间的合作,将难以开展前瞻性研究以探讨不同治疗方式或技术的疗效。
综上所述,本中心报道的3例CIRT治疗眼眶恶性肿瘤,获得了满意的1年OS率、LC率及PFS率,未观察到严重的急性、晚期毒性反应。对于不可手术、术后残留、术后复发眼眶恶性肿瘤,CIRT碳离子放疗是一种疗效好且不良反应小的治疗方法。
参考文献
[1]Pol JN, Patil DB, Desai SS, et al. Malignant recurrent orbital solitary fibrous tumor[J]. Indian J Pathol Microbiol, 2023, 66(4):819-822.
[2]Biswas A, Kumar R, Bakhshi S, et al. Multimodal Management of Congenital Orbital Malignant Rhabdoid Tumor: Review of Literature and Report of a Rare Case[J]. J Pediatr Hematol Oncol, 2020, 42(3):228-233.
[3]Poudyal P, Hamal D, Shrestha P. Orbital Tumors and Tumor like Lesions: A Hospital Based Study[J]. J Nepal Health Res Counc, 2022, 20(1):26-32.
[4]Tom A, Bell D, Ford JR, et al. Malignant Mixed Tumor (Carcinoma Ex Pleomorphic Adenoma) of the Lacrimal Gland[J]. Ophthalmic Plast Reconstr Surg, 2020, 36(5):497-502.
[5]Joseph AK, Guerin JB, Eckel LJ, et al. Imaging Findings of Pediatric Orbital Masses and Tumor Mimics[J]. Radiographics, 2022, 42(3):880-897.
[6]Jones KE, Patel A, Kunesh MG, et al. Malignant peripheral nerve sheath tumor of the orbit: a case report and review of the literature[J]. Orbit, 2022, 41(5):642-646.
[7]Chen X, Badian RA, Hynne H, et al. Alterations in meibomian glands in patients treated with intensity-modulated radiotherapy for head and neck cancer[J]. Sci Rep, 2021, 11(1):22419.
[8]Wu F, Chen B, Dong D, et al. Phase 2 Evaluation of Neoadjuvant Intensity-Modulated Radiotherapy in Centrally Located Hepatocellular Carcinoma: A Nonrandomized Controlled Trial[J]. JAMA Surg, 2022, 157(12):1089-1096.
[9]Reshef ER, Bleier BS, Freitag SK. The Endoscopic Transnasal Approach to Orbital Tumors: A Review[J]. Semin Ophthalmol, 2021, 36(4):232-240.
[10]Ye-Zhu C, Muñoz-Ramón PV, Barrancos C, et al. Orbital myopericytoma: an unusual tumor in an unusual location[J]. Orbit, 2022, 41(4):502-505.
[11]Tooley AA, Maher M, Cooper C, et al. Reliability of 3 Strategies of Orbital Tumor Volume Measurement Using Phantom Modeling[J]. Ophthalmic Plast Reconstr Surg, 2021, 37(3S):S33-S38.
[12]Zhou Q, Liu Y, Wang F, et al. A giant orbital solitary fibrous tumor treated by surgical excision: a case report and literature review[J]. Diagn Pathol, 2023, 18(1):59.
[13]Feu-Basilio S, Matas J, Dotti-Boada M, et al. Orbital TFE3-Rearranged Perivascular Epithelioid Cell Tumor: A Case Report and Review of the Literature[J]. Am J Dermatopathol, 2021, 43(12):e263-e266.
[14]Orapan Aryasit, Passorn Preechawai, Chakree Hirunpat, et al. Factors related to survival outcomes following orbital exenteration: a retrospective, comparative, case series[J]. BMC Ophthalmol, 2018, 18(1):186.
[15]Aki Hirai, Atsushi Mizota, Seiichiro Mine, et al. Two cases of orbital adenocarcinoma treated with heavy charged carbon particle irradiation[J]. Graefes Arch Clin Exp Ophthalmol, 2005, 243(6):610-614.
[16]Huang SF, Lin JC, Shiau AC, et al. Optimal tumor coverage with different beam energies by IMRT, VMAT and TOMO: Effects on patients with proximal gastric cancer[J]. Medicine (Baltimore), 2020, 99(47):e23328.
[17]Pointreau Y, Moreau J, Vendrely V, et al. Impact of IMRT for neoadjuvant rectal cancer?[J]. Cancer Radiother, 2022, 26(6-7):865-870.
[18]Itonaga T, Mikami R, Okubo M, et al. Prognostic impact of solid tumor component diameter in early-stage non-small cell lung carcinoma treated with intensity-modulated fractionated radiotherapy: a retrospective analysis impact of solid tumor component diameter in NSCLC treated with IMRT[J]. Br J Radiol, 2020, 93(1109):20191027.
[19]Liu X, Wu B, Huang J, et al. Tumor factors associated with in-field failure for nasopharyngeal carcinoma after intensity-modulated radiotherapy[J]. Head Neck, 2022, 44(4):876-888.
[20]Killock D. Recurrent nasopharyngeal carcinoma: hyperfractionation of IMRT improves outcomes[J]. Nat Rev Clin Oncol, 2023, 20(5):283.
[21]Takahashi D, Demizu Y, Koto M, et al. Multicenter study of re-irradiation using carbon-ions for head and neck malignancies after photon radiotherapy[J]. Cancer Med, 2022, 11(19):3593-3601.
[22]Liu X, Yue H, Jiang S, et al. Clinical features and prognosis of patients with metastatic ocular and orbital melanoma: A bi-institutional study[J]. Cancer Med, 2023, 12(15):16163-16172.
[23]Susko MS, Lazar AA, Dhar S, et al. Improved Tumor Control Related to Radiotherapy Technological Development for Hypopharyngeal Cancer[J]. Laryngoscope, 2021, 131(2):E452-E458.
[24]陈宇鹏, 史路林, 王瑜玉, 等. GeV重离子束辐照LiF引起的晶体内部结构改变[J]. 物理学报, 2024, 73(15):111-117.
[25]Shih CY, Huang WL, Chiang IT, et al. Biocompatible hole scavenger-assisted graphene oxide dots for photodynamic cancer therapy[J]. Nanoscale, 2021, 13(18):8431-8441.

